Reinvestment Partners has been on a mission to make its produce-prescription program a standard healthcare service that can be reimbursed by insurers. The results of its latest clinical trial move it one step closer to that goal, with some caveats.
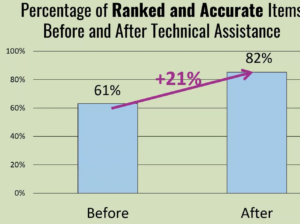
The Durham, N.C.-based nonprofit announced in November that a randomized test of its Eat Well produce prescription program reduced blood pressure among participants, in addition to improving food security. The results were significant, showing blood pressure going down by about 5.4 millimeters of mercury – much more than the 1- to 2-millimeter of mercury difference deemed necessary to markedly lower rates of heart attacks and strokes among the general public.
The results offer another proof-point that Food is Medicine interventions can be prescribed with confidence, making the trial “a seminal, landmark case,” said Peter Skillern, CEO of Reinvestment Partners. At the same time, Skillern recognizes that over the long term there is still much more work to be done before Food is Medicine services are fully embedded into healthcare.

Reinvestment Partners has run one of the largest produce prescription programs in the country since 2017, growing and adapting it over the years as funding and partnerships have evolved. One of its mainstay activities is to continue testing and evaluating various aspects of the programs to ensure they are meeting business, regulatory and healthcare requirements.
While everyone seems to agree that nutritious food is beneficial to health, the business case for Food is Medicine has not necessarily been proven to the healthcare and insurance sectors. “The moral argument is very strong,” Skillern noted. “But the business argument requires us to show that we’re delivering that intervention in a way that science can back up, that it works.”
For that reason, Reinvestment Partners has been a relentless tester of Food is Medicine interventions. The study of blood pressure was one of about 15 serious studies it has undertaken over the years to evaluate different aspects of produce prescriptions, and it has many more such studies in the pipeline. “We know it works,” Skillern said. “But we’ve got to convince the payers, Congress, Medicaid, and the people who are in charge that this is a good investment of money.”
There are so many questions to be answered: How much produce should be in a dosage? How many months should an intervention last? How should the health benefit be measured? How long should the health benefit last? What’s the best form of providing assistance? How should the financial return be measured? Over what timeframe? “There are a wide range of questions that are being asked by the research,” Skillern noted. “Sometimes it’s a yes, and sometimes it’s a no. It’s part of the process.”
Outcomes from Reinvestment Partners’ most recent study included the finding that produce prescription cards were more effective than two other interventions: food boxes and nutrition education. While both the food boxes and the produce prescription cards increased food security and brought down blood pressure, the prescription cards reduced blood pressure by more. The nutrition education program, meanwhile, did not have much of an impact along either measure.
The produce prescription program provided $40 each month on a prepaid debit card that participants could use to shop for fruits and vegetables at a range of grocery stores and other retailers. Funds could only be used to purchase fresh, frozen or canned fruits and vegetables that do not have added salt, sugar or fats. The food box, meanwhile, provided $115 worth of healthy food monthly. The less expensive card program was more effective than the box program, Skillern surmised, because the cards provided more “agency and choice” versus the food boxes.
Produce prescription cards also offer the benefit of integrating nicely within the existing commercial food network, since benefit cards are widely accepted at places where people shop, making them easy to scale, while food boxes need to be sourced, packed and delivered. Skillern emphasized, however, that food boxes still need to be in the solutions mix, since they may be the only appropriate solution for people who can’t make it to the store.
Skillern praised food banks for promoting the positive impact of food security on population health. An area that still needs work is for hunger relief systems to seamlessly integrate with health care systems, especially in terms of taking in and closing the loop on referrals. “If we’re trying to build out a system that incorporates food banks, that’s an area that will need to be developed,” he said. – Chris Costanzo
Like what you’re reading?
Support Food Bank News